KRAS
The Undruggable Switch
The most frequently mutated oncogene in human cancer — and for nearly forty years the best chemists alive called it “undruggable.”
The walkthrough
Beat by beat

HOOK
0:33
01HOOK
It's the single most frequently mutated oncogene in all of human cancer `F1` — the engine behind roughly nine out of ten pancreatic tumors `F2`. We've known almost exactly what it does since 1982. And for nearly forty years after that, the best chemists in the world could not lay a glove on it. They simply called it undruggable `F3`. This is the story of KRAS.
02THE NAME
The name is a fossil. KRAS stands for Kirsten Rat Sarcoma `F4` — because the gene was first glimpsed not in a person, but in a virus that gave rats cancer, isolated by Werner Kirsten in 1967 `F5`. The human version sits on the short arm of chromosome 12 `F6`. And it builds something almost absurdly small: a single protein that works as a molecular switch, telling a cell when to grow `F7`.
03THE HUNT
In the early 1980s, three labs were racing to do something no one ever had — pull a cancer-causing gene straight out of a human tumor. Robert Weinberg at MIT. Michael Wigler at Cold Spring Harbor. Mariano Barbacid at the National Cancer Institute `F8`. They succeeded almost at once. The very first gene came out of a bladder tumor — and it turned out to be a ras gene `F9`. KRAS itself surfaced right behind it, in cancers of the lung and the colon `F10`.
04THE METHOD
Then came the shock. In 1982, Weinberg's and Barbacid's teams published back-to-back, in the very same issue of Nature `F11`. The only difference between the healthy gene and the cancer gene was a single letter of DNA — one base, changing one amino acid: the twelfth, from glycine to valine `F12`. That was all it took to turn a normal gene into an oncogene. And KRAS, it turned out, carries the exact same Achilles' heel, in the exact same place — codon twelve `F13`.
05THE MECHANISM (hero)
Here is what that switch actually does. Normal KRAS flips between two states — off when it holds a molecule called GDP, on when it grabs GTP `F14`. One set of helper proteins flips it on; another flips it off, by forcing it to burn its fuel `F15`. The whole shut-off step depends on that twelfth amino acid being glycine — the smallest building block there is, with no side chain at all. Swap in anything bulkier, and the off-switch machinery no longer fits `F16`. So the switch jams on `F17`. And a cell whose KRAS is stuck on hears a single command, forever: grow, divide, grow `F18`.
06THE STAKES
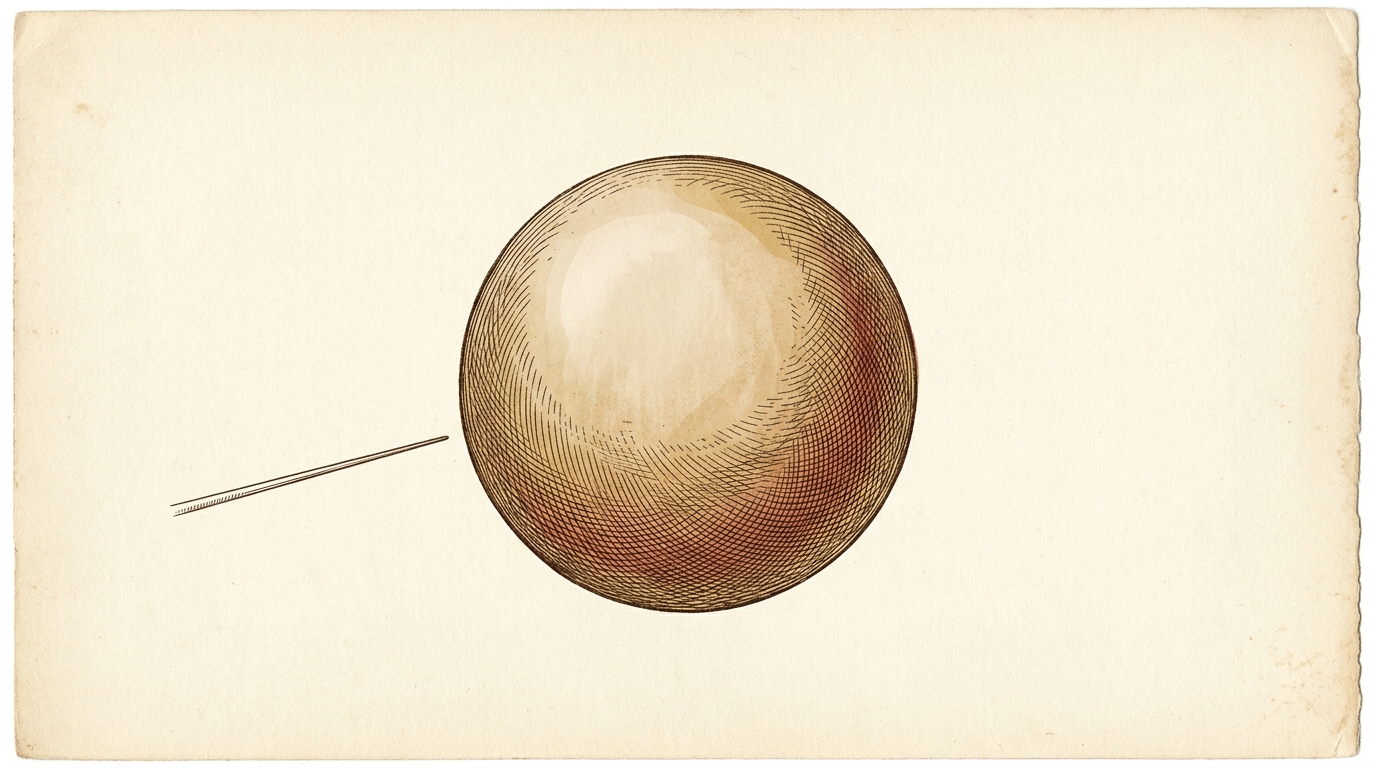
So why not just build a drug to force it back off? For three decades, no one could. KRAS is a smooth, almost featureless ball, with no deep pocket for a drug to grab onto `F19`. And it clamps its fuel so tightly, at picomolar strength, that no molecule could ever compete it away `F20`. Meanwhile pancreatic cancer, ninety percent of it driven by this one jammed switch, remained among the deadliest diagnoses in all of medicine `F21`.
07THE TURN
The break came in 2013. Kevan Shokat's lab at UCSF found a pocket nobody knew was there — a cleft that only opens on one specific mutant, called G12C, where that twelfth amino acid happens to become a cysteine `F22`. They designed a molecule that snaps permanently into it `F23`. By 2021, the first KRAS drug in history was approved — a second followed in 2022 `F24`. But there was a cruel catch. G12C is common in lung cancer — and almost absent in the pancreas, where the culprit is a different letter, G12D `F25`. The breakthrough barely reached the patients who needed it most.
082026: PANCREAS
Which brings us to now. The covalent drugs had to catch KRAS in the off state and pin it shut — and only when it carried that one rare cysteine `F23` `F25`. The newest drug does the opposite. Daraxonrasib grabs KRAS while it's still on: it acts like a molecular glue, latching onto a helper protein inside the cell and using it to clamp the active switch, smothering its signal `F31`. And because it no longer needs that cysteine, it covers the whole family of pancreatic mutations at once `F26`. In June 2026, that first large pancreatic-cancer trial reported out: it nearly doubled median survival — about thirteen months versus six and a half `F27`. It is not a cure, and it is not yet approved `F28`. But after forty years, the undruggable gene is finally — measurably — on the back foot.
09TIMELINE + SIGN-OFF
A rat virus in 1967. A single misplaced letter in 1982. A hidden pocket in 2013. And in 2026, the first real gain in survival, in the cancer that needed it most. One stubborn switch — and the long campaign to finally turn it off. — The Gene Channel.
The write-up
In one line: A single change at codon 12 jams KRAS — the most-mutated oncogene in human cancer — permanently "on"; smooth and pocketless, it defied drug-makers for nearly forty years, until a hidden cleft (2013) gave us the first KRAS drugs and, in 2026, a "molecular glue" finally moved survival in pancreatic cancer.
The gene
KRAS is the single most frequently mutated oncogene in all of human cancer, and the engine behind roughly nine out of ten pancreatic tumors. The name is a fossil: Kirsten Rat Sarcoma, after the rat-cancer virus in which the gene was first glimpsed, isolated by Werner Kirsten in 1967. The human gene sits on the short arm of chromosome 12 and builds something almost absurdly small — a single protein that works as a molecular on/off switch, telling a cell when to grow.
The hunt
In the early 1980s, three labs raced to do something no one ever had: pull a cancer-causing gene straight out of a human tumor — Robert Weinberg at MIT, Michael Wigler at Cold Spring Harbor, and Mariano Barbacid at the National Cancer Institute. The very first one came out of a bladder tumor and turned out to be a ras gene; KRAS surfaced right behind it, in cancers of the lung and colon. In 1982, Weinberg's and Barbacid's teams published back-to-back in the same issue of Nature: the only difference between the healthy gene and the cancer gene was a single letter of DNA — one base at codon 12, changing glycine to valine. KRAS, it emerged, carries the same Achilles' heel in the same place.
The mechanism
Normal KRAS flips between two states — off when it holds GDP, on when it grabs GTP. One set of helper proteins flips it on; another flips it off by forcing it to burn its fuel. That shut-off step depends on the twelfth amino acid being glycine — the smallest building block there is, with no side chain at all. Swap in anything bulkier and the off-switch machinery no longer fits, so the switch jams on, and the cell hears a single command forever: grow, divide, grow.
The stakes, and the frontier
For three decades no one could force the switch back off. KRAS is a smooth, almost featureless ball with no deep pocket for a drug to grab, and it clamps its fuel so tightly — at picomolar strength — that no molecule could compete it away. Meanwhile pancreatic cancer, ~90% of it driven by this one jammed switch, stayed among the deadliest diagnoses in medicine. The break came in 2013, when Kevan Shokat's lab at UCSF found a cryptic pocket that opens only on the G12C mutant, where codon 12 becomes a cysteine; a molecule designed to snap covalently into it became the first KRAS drug in history (approved 2021, a second in 2022). But G12C is common in lung cancer and nearly absent in the pancreas, where the culprit is G12D — so the breakthrough barely reached the patients who needed it most. The newest drug, daraxonrasib, does the opposite: it grabs KRAS while it is still on, acting like a molecular glue that recruits a helper protein to clamp the active switch and smother its signal — and because it no longer needs the rare cysteine, it covers the whole family of pancreatic mutations. In June 2026 the first large pancreatic-cancer trial reported it nearly doubled median survival (~13 months vs ~6.5). It is not a cure, and not yet approved — but after forty years, the undruggable gene is measurably on the back foot.
Sources
Full claim-by-claim evidence is in references.md. Primary anchors:
- NCI — RAS Initiative — prevalence, "undruggable" history, drug landscape
- NCBI Gene 3845 — KRAS — locus, gene/protein identity
- PMC4355017 — RAS biology and the GDP/GTP switch
- PMC11012482 — KRAS therapeutics and the G12C pocket
- Nature (2013) PMID 24256730 — Shokat: the cryptic switch-II pocket on G12C
Accuracy note: The 1982 "single-letter" discovery the episode dramatizes was made in HRAS (from a bladder-carcinoma line), not KRAS; the narration keeps it as "the gene" and bridges to KRAS because KRAS carries the identical codon-12 lesion. The 2026 daraxonrasib survival figure comes from a reported trial — the drug is not a cure and is not yet approved.
The evidence
Every claim, sourced
Each [F#] you hear in the film links to the source it came from. Nothing gets narrated until every one is checked and signed off.
Sign-off
- PhD sign-off — facts above are correct; the four traps are stated correctly in
script.md. - Numbers/dates verified (or kept qualitative): 1967, 1982 (Nature back-to-back), 2013 (Shokat), 2021/2022 (FDA G12C), June 2026 (RASolute 302: 13.2 vs 6.6 mo, HR 0.40). Re-confirm daraxonrasib approval status at lock — fastest-moving fact.
**Gate OPEN** (2026-06-11, producer sign-off) → narration + assets cleared. Re-confirm daraxonrasib approval status before the final render lock.
- F1
KRAS is the single most frequently mutated oncogene in human cancer.
Standard framing across the RAS literature; KRAS is the most commonly mutated of the RAS isoforms, itself the most-mutated oncogene family.
- F2
Drives roughly nine out of ten pancreatic tumors (~90%).
Activating KRAS mutation found in ~90% (range ~85–95%) of pancreatic ductal adenocarcinoma.
- F3
We've understood it since 1982, yet for ~40 yrs it resisted drugging — "undruggable."
RAS identified as human oncogene 1982; directly undruggable until the 2013 pocket / 2021 first drug. Shokat 2013 frames RAS as having "eluded drug discovery efforts for more than three decades."
- F4
KRAS = "Kirsten Rat Sarcoma" (viral oncogene homolog).
Named for the Kirsten rat sarcoma virus; "ras" = rat sarcoma.
- F5
First glimpsed in a virus that gave rats cancer — isolated by Werner Kirsten in 1967.
Kirsten & Mayer described the Kirsten murine sarcoma virus (in rats) in 1967. (Cf. Harvey 1964 → HRAS.)
- F6
The human gene sits on the short arm of chromosome 12.
KRAS cytoband 12p12.1 (chr12 short arm). (Not 11 — that's HRAS.)
- F7
It builds one small protein — a molecular switch that tells a cell when to grow.
KRAS encodes a ~21-kDa small GTPase ("p21"), a binary on/off switch in growth-factor signal transduction.
- F8
Early-1980s race: Weinberg (MIT), Wigler (Cold Spring Harbor), Barbacid (NCI) to pull a cancer gene from a human tumor.
Three groups independently isolated the first human transforming oncogene by NIH-3T3 transfection.
- F9
The first gene came out of a bladder tumor — and was a ras gene.
The T24/EJ bladder-carcinoma transforming gene = HRAS (a ras gene). Trap: this gene was HRAS, not KRAS — narration says only "a ras gene."
- F10
KRAS itself surfaced right behind it, in lung and colon cancers.
Der/Krontiris/Cooper mapped the lung carcinoma transforming gene to Kirsten/KRAS (bladder→Harvey/HRAS); KRAS also cloned from colon lines (e.g. SW480).
- F11
In 1982 Weinberg's and Barbacid's teams published back-to-back in the same issue of Nature.
Companion papers, Nature vol. 300 (1982): Tabin et al. (Weinberg) pp.143–149; Reddy et al. (Barbacid) pp.149–152.
- F12
The difference was a single base — one amino acid, the 12th, glycine→valine.
A single G→T substitution swaps Gly12→Val in p21, conferring transforming activity (T24/EJ HRAS).
- F13
KRAS carries the same Achilles' heel at the same place — codon 12.
Codon 12 is the dominant oncogenic hotspot in KRAS across cancers (esp. pancreas). Trap stated carefully: KRAS codon-12 mutations are to varied residues (G12D/V/R…), not specifically the HRAS G12V — script says only "the same spot, codon 12."
- F14
KRAS flips between off (GDP-bound) and on (GTP-bound).
The RAS GTPase cycles: GDP-bound = inactive/off, GTP-bound = active/on.
- F15
Helper proteins flip it on; others flip it off by forcing it to burn its fuel.
GEFs (e.g. SOS1) catalyze GDP→GTP exchange (on); GAPs (e.g. NF1, p120RasGAP) accelerate GTP hydrolysis ~10⁵-fold (off).
- F16
The off-switch needs Gly12 (smallest, no side chain); a bulkier residue blocks it.
Gly12 sits in the P-loop at the active site; with no side chain it leaves room for the GAP "arginine finger"/transition state. Bulkier substitutions sterically block GAP-stimulated hydrolysis.
- F17
So the switch jams on.
Codon-12 mutants resist GAP-mediated hydrolysis → KRAS stays GTP-bound (constitutively active).
- F18
A cell with KRAS stuck on hears one command: grow, divide.
Active KRAS constitutively fires RAF→MEK→ERK (and PI3K→AKT), driving proliferation/survival.
- F19
KRAS is a smooth, near-featureless ball — no deep pocket for a drug.
Lack of deep hydrophobic surface pockets (outside the nucleotide site) is the classic reason for "undruggable."
- F20
It clamps its fuel at picomolar strength — nothing could compete it away.
KRAS binds GDP/GTP with picomolar affinity against ~mM cellular nucleotide, ruling out nucleotide-site competition.
- F21
Pancreatic cancer — 90% driven by this switch — stayed among the deadliest diagnoses.
~90% KRAS-mutant PDAC; pancreatic cancer 5-yr survival ~13%, among the lowest of major cancers.
- F22
2013, Shokat lab (UCSF) found a hidden pocket on the G12C mutant (12th residue = cysteine).
Ostrem/Peters/Shokat discovered the cryptic switch-II pocket; the G12C mutation supplies a reactive cysteine at residue 12.
- F23
They designed a molecule that snaps permanently into it.
Covalent (irreversible) inhibitor bonds the mutant Cys12; allosterically favors the inactive GDP/off state, blocking effector engagement.
- F24
By 2021 the first KRAS drug was approved; a second in 2022.
Sotorasib (Lumakras) FDA accelerated approval May 28 2021; adagrasib (Krazati) Dec 12 2022 — both KRAS G12C NSCLC.
- F25
G12C is common in lung cancer, nearly absent in pancreas — where the culprit is G12D.
Pancreatic KRAS: G12D ~40%, G12V ~33%, G12R ~17%, G12C only ~1–2%; G12C dominates lung adeno (~40% of KRAS-mut).
- F26
A new generation hits KRAS while it's ON; the leading one, daraxonrasib, covers the whole pancreatic mutation family.
Daraxonrasib (RMC-6236, Revolution Medicines) = oral RAS-multiselective RAS(ON) inhibitor (tri-complex w/ cyclophilin A), targeting active GTP-bound RAS incl. G12D/V/R.
- F27
June 2026, first large pancreatic trial: nearly doubled median survival — ~13 mo vs ~6.5.
RASolute 302 (NCT06625320) Phase 3, 2nd-line metastatic PDAC: median OS 13.2 vs 6.6 mo (RAS G12 population), HR 0.40; ASCO 2026 Plenary (LBA5) + NEJM.
- F28
Not a cure, and not yet approved.
As of 2026-06-11 daraxonrasib is investigational (FDA Breakthrough Therapy June 23 2025; NDA via CNPV pilot pending); even 13 mo median OS = most patients still die <2 yr. No KRAS drug is FDA-approved for pancreatic cancer.
- F29
(seg-04 on-screen) the discovery mutation: codon 12 GGC → GTC, glycine → valine.
The T24/EJ bladder HRAS oncogene carries a single G→T at position 35 (2nd base of codon 12): GGC (Gly) → GTC (Val) =
c.35G>T,p.Gly12Val. (This is the HRAS discovery lesion; KRAS shares the codon-12 hotspot — see F13.) - F30
(seg-04 on-screen) read by Maxam–Gilbert (Gilbert) chemical sequencing.
The 1982 ras point mutations were determined by both dideoxy and the Maxam–Gilbert chemical-sequencing procedure — depict/label as "chemical sequencing (Maxam–Gilbert)", not the sole method.
- F31
(seg-08) daraxonrasib grabs KRAS while it's ON — a "molecular glue" that binds a helper protein and clamps the active switch, smothering its signal; needs no cysteine, so it covers the whole G12 family.
RMC-6236 is a noncovalent RAS(ON) multi-selective inhibitor: it obligately binds the chaperone cyclophilin A first, forming a tri-complex with active, GTP-bound RAS that sterically blocks RAF/MEK/ERK effector engagement; active across G12D/V/R — unlike the covalent G12C OFF-state inhibitors (F22/F23) which bond the mutant cysteine and trap the inactive state.