DMD
The Longest Read
The largest gene in your body takes sixteen hours to read — and its sheer size is what makes Duchenne the most common fatal muscle disease of childhood.
The walkthrough
Beat by beat

HOOK
0:33
01HOOK
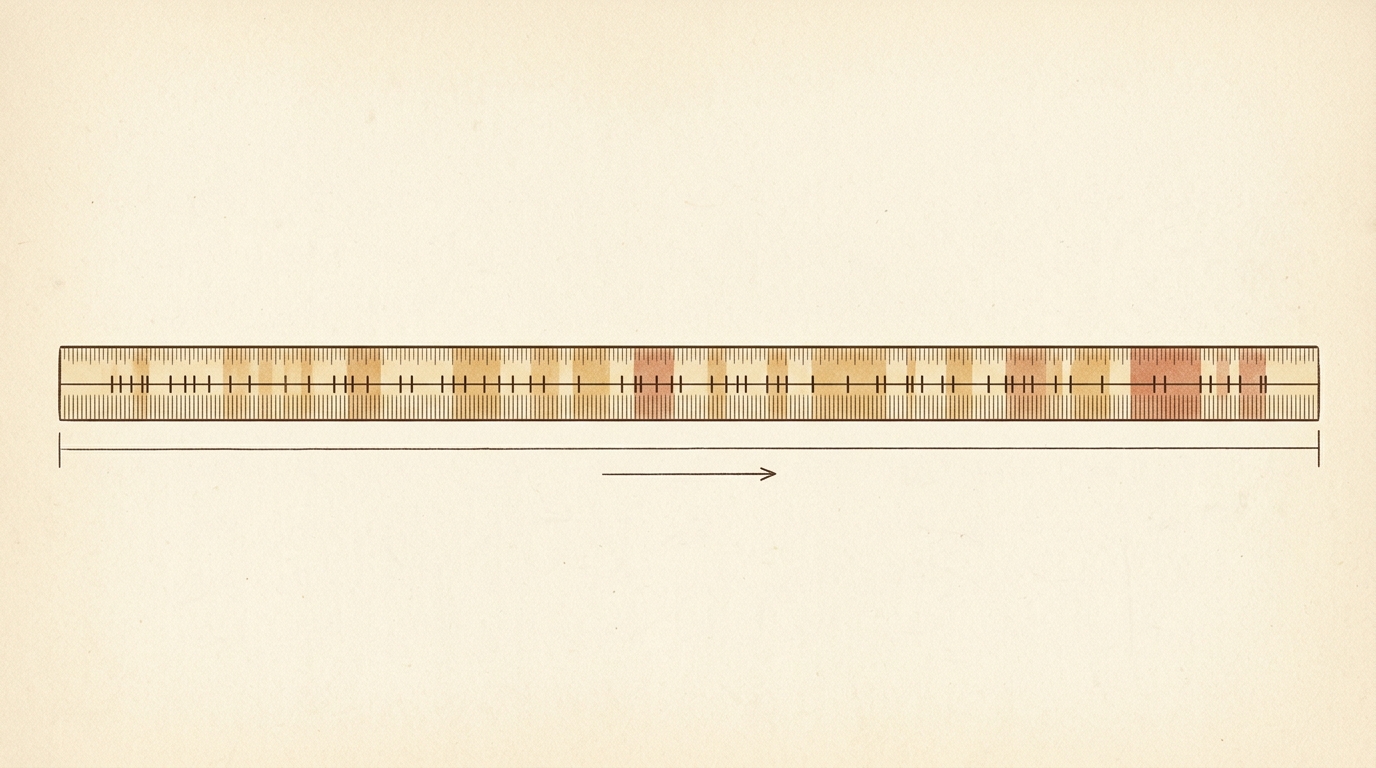
In your cells right now, one gene is being read that will take sixteen hours to finish `F1`. Most genes clock in at minutes. DMD spans more than two million base pairs — the largest known gene in the human genome `F2`. Its size is its vulnerability: the longer the target, the more often mutation strikes `F3`. One in every five thousand boys is born with a deletion here. And without the protein it makes, muscles don't just weaken — they tear themselves apart.
02THE NAME
The gene sits on the X chromosome at band Xp21.2 `F4`, and it makes dystrophin — a long, rod-shaped protein that lines the inside of every muscle cell `F5`. Think of it as a molecular shock absorber: it links the fiber's internal skeleton to the surrounding membrane and the extracellular scaffold beyond `F6`. Every contraction generates force; dystrophin distributes that force so the membrane survives. Lose it, and the fiber quietly destroys itself with each beat.
03THE HUNT
In the early 1980s, the gene responsible for Duchenne muscular dystrophy was known only by what it took. In 1986, Louis Kunkel's group at Harvard used positional cloning — methodically narrowing the disease's address on the X chromosome — and pulled out a gene unlike anything they had seen `F7`. The following year, Eric Hoffman named the protein it encoded: dystrophin, for the dysfunction that follows its absence `F8`.
04THE READING FRAME RULE
But the gene's size created a puzzle. Two boys could each carry a large deletion in DMD and have completely different fates — one severe, wheelchair-bound by twelve; the other barely noticing weakness until adulthood `F9`. The difference wasn't the size of the deletion. It was the reading frame `F10`. The gene is assembled from 79 exons `F11`, and the code is read in three-letter words. Delete a stretch that keeps the remaining exons in-frame, and the cell still assembles a shorter, partly working dystrophin — that's Becker muscular dystrophy, the milder form. Delete a stretch that shifts every downstream codon out of phase, and the output is nonsense — the protein lost entirely. That's Duchenne `F12`.
05THE MECHANISM (hero)
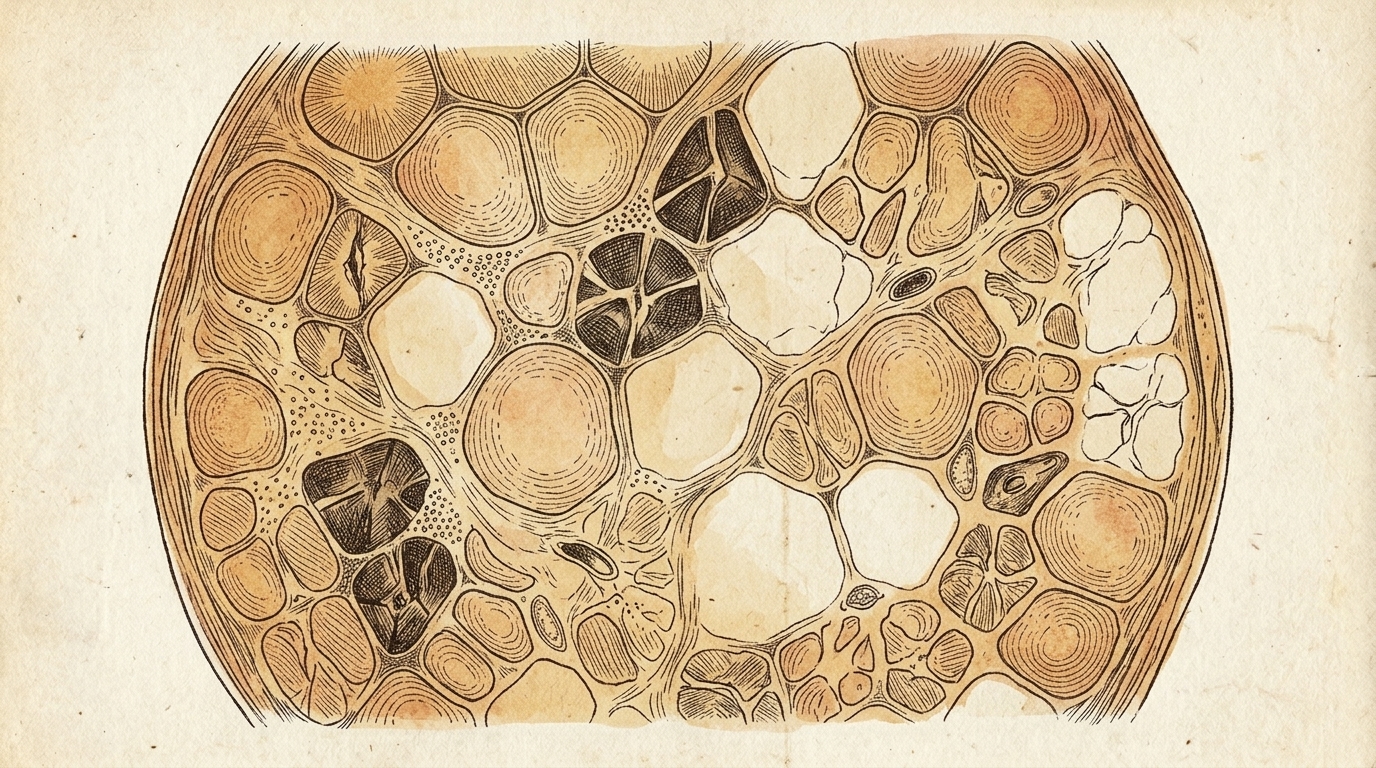
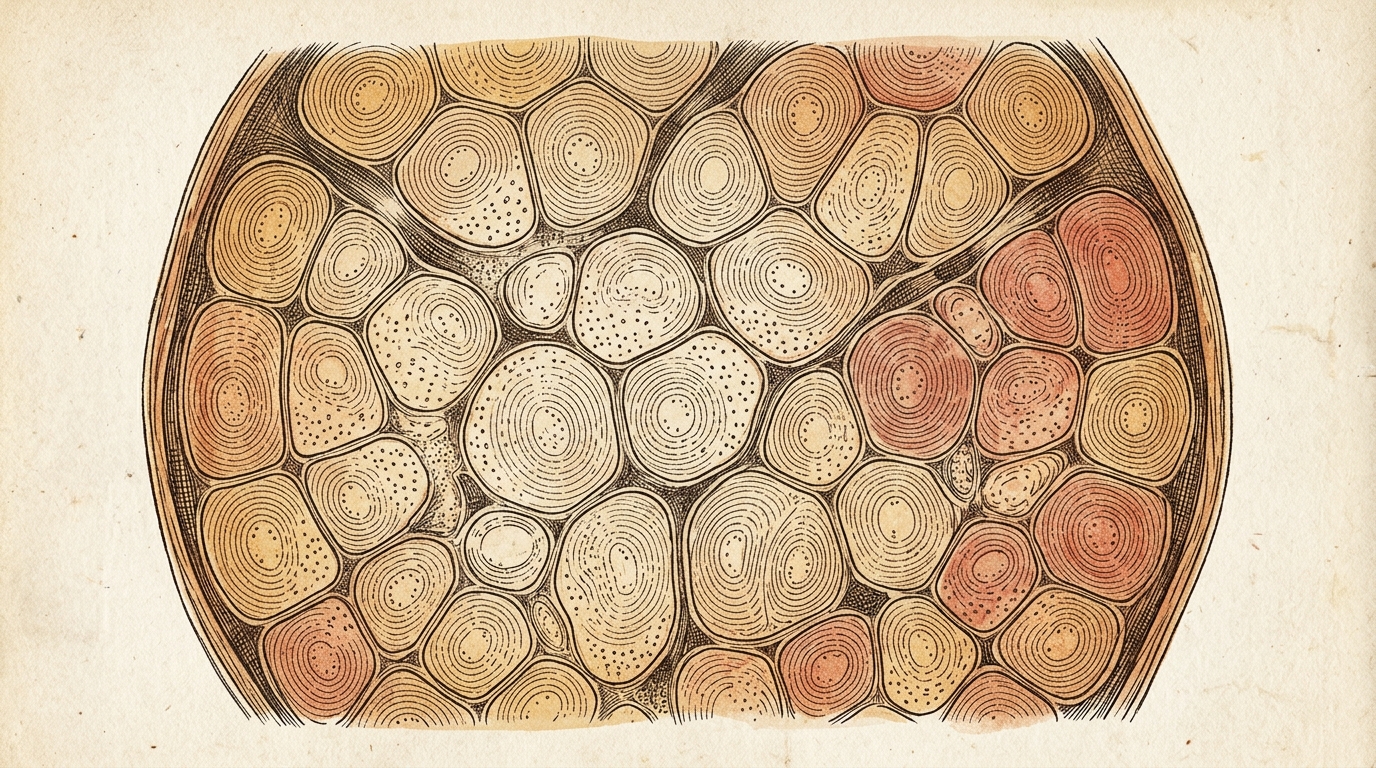
Without dystrophin, every contraction micro-tears the muscle membrane `F13`. The body's repair systems fight back, but they fall progressively behind. Muscle fibers are replaced by fat and connective tissue `F14` until contraction is no longer possible. The heart and diaphragm follow the same trajectory. Boys with Duchenne typically lose independent walking in their early teens `F15`.
06THE STAKES
Duchenne muscular dystrophy is the most common fatal muscle disease of childhood `F15b`. Before corticosteroids extended prognosis, median survival barely reached the mid-twenties `F16`. With modern supportive care — steroids, ventilators, cardiac medications — many patients now live into their thirties and beyond. But living longer with the disease is not the same as treating it.
07THE OPEN THREAD
The reading frame pointed toward a fix. If out-of-frame deletions cause Duchenne, then forcing the splicing machinery to skip one additional exon — jumping over the deletion site to land back in frame — could convert a Duchenne mutation toward the milder Becker pattern `F17`. The first exon-skipping drug, eteplirsen, targeting exon 51, was approved in 2016 `F18`. Three more antisense oligonucleotide drugs have followed, each targeting a different exon, together covering roughly a third of all DMD patients. Then, in 2023, the FDA approved the first gene therapy for the disease: delandistrogene moxeparvovec (Elevidys) — a miniaturized dystrophin gene delivered directly into muscle by a viral vector `F19`. For the youngest patients treated before significant fibrosis, it can restore what the deletion took.
08TIMELINE + SIGN-OFF
Guillaume Duchenne described the disease in 1868 `F20`. The gene was found in 1986. The reading frame explained the variability in 1988. The first drug was approved a hundred and twenty-eight years after the first patient. DMD is the story of what happens when a gene is too large to stay intact — and what happens when scientists understand why it breaks well enough to start writing the fix. — The Gene Channel.
The write-up
In one line: DMD is the largest gene in the human genome — over two million bases, ~16 hours to transcribe — and its size is its weakness: without the shock-absorber protein dystrophin, muscle tears itself apart with every contraction; the "reading-frame rule" explains why some deletions cause severe Duchenne and others mild Becker, and it pointed the way to exon-skipping drugs and, in 2023, the first gene therapy.
The gene
DMD sits on the X chromosome at band Xp21.2 and spans more than two million base pairs — the largest known gene in the human genome, so long that a single copy takes about sixteen hours to transcribe. It encodes dystrophin, a long, rod-shaped protein that lines the inside of every muscle fiber and acts as a molecular shock absorber: it links the fiber's internal skeleton to the surrounding membrane and the scaffold beyond, distributing the force of each contraction so the membrane survives. The gene's size is its vulnerability — the longer the target, the more often mutation strikes — and roughly one in five thousand boys is born with a deletion here.
The hunt
In the early 1980s the gene behind Duchenne muscular dystrophy was known only by what it took. In 1986, Louis Kunkel's group at Harvard used positional cloning — methodically narrowing the disease's address on the X chromosome — to pull out a gene unlike anything seen before. The following year, Eric Hoffman named the protein it encodes dystrophin, for the dysfunction that follows its absence.
The mechanism
The gene's size created a puzzle: two boys could each carry a large deletion in DMD yet have completely different fates — one wheelchair-bound by twelve, the other barely noticing weakness into adulthood. The difference wasn't the size of the deletion but the reading frame. The gene is assembled from 79 exons, read in three-letter words. A deletion that keeps the remaining exons in-frame still yields a shorter, partly working dystrophin — the milder Becker muscular dystrophy. A deletion that shifts every downstream codon out of phase produces nonsense and no protein — Duchenne. Without dystrophin, every contraction micro-tears the membrane; repair systems fall behind, and muscle is replaced by fat and connective tissue until contraction fails. The heart and diaphragm follow the same path.
The stakes, and the frontier
Duchenne is the most common fatal muscle disease of childhood; before corticosteroids, median survival barely reached the mid-twenties. Modern supportive care — steroids, ventilators, cardiac medications — now carries many patients into their thirties and beyond, but that is living with the disease, not treating it. The reading-frame rule pointed toward a fix: force the splicing machinery to skip one more exon, jumping over the deletion to land back in frame, converting a Duchenne mutation toward the milder Becker pattern. The first exon-skipping drug, eteplirsen (exon 51), was approved in 2016; three more antisense oligonucleotides have followed, together covering roughly a third of patients. Then in 2023 the FDA approved the first gene therapy for the disease — delandistrogene moxeparvovec (Elevidys), a miniaturized dystrophin gene delivered into muscle by a viral vector — which, for the youngest patients treated before significant fibrosis, can begin to restore what the deletion took.
Sources
Full claim-by-claim evidence is in references.md. Primary anchors:
- NCBI Gene 1756 — DMD — locus, gene size, dystrophin
- UniProt P11532 — dystrophin — protein structure/function
- Ervasti & Campbell (1991) Cell — PMID 1655922 — dystrophin links cytoskeleton to membrane/ECM
- Emery (1991) — PMID 2060820 — incidence, clinical course
- MedlinePlus — DMD — overview, Duchenne vs Becker
Accuracy note: Severity tracks the reading frame, not the deletion's size — in-frame deletions → milder Becker, frameshifting deletions → Duchenne (the rule Monaco/Kunkel formalized in 1988). Exon-skipping doesn't "repair" the gene; it coaxes splicing to restore the frame, aiming to shift Duchenne toward a Becker-like, partly functional dystrophin. Elevidys delivers a miniaturized (micro-)dystrophin, not the full-length protein.
The evidence
Every claim, sourced
Each [F#] you hear in the film links to the source it came from. Nothing gets narrated until every one is checked and signed off.
Sign-off
- PhD sign-off — facts above are correct; traps ⚠️ are stated correctly in
script.mdand this table. - Numbers/dates verified (F1 transcription time, F3 prevalence range, F15 ambulatory loss age, F16 survival).
- Reading-frame rule framing (F10/F12) — "lost entirely" for out-of-frame accepted as correct for the muscle context.
Gate OPEN → narration + render may proceed. (Signed off 2026-06-13.)
- F1
Transcription of DMD takes ~16 hours
Tennyson et al. 1995 (Nat Genet): "The human dystrophin gene requires 16 hours to be transcribed and is cotranscriptionally spliced." Direct measurement by nuclear run-on and intron-retention assays.
- F2
DMD spans more than two million base pairs — largest known human gene
PMC5664101 (L12, confirmed via paperclip): "spanning over 2400 kb on the X-chromosome. The gene is comprised of 79 exons." Also NCBI Gene ID 1756: ~2,220,233 bp (GRCh38).
- F3
Large size → elevated mutation rate; ~one in 5,000 male births
PMC11818380 (L9, confirmed via paperclip): "approximately one in 5000 male births worldwide, irrespective of race." Range in literature: 1:3,500–1:5,000. Narration uses 1 in 5,000 (conservative).
- F4
DMD locus: chromosome Xp21.2
NCBI Gene (ID 1756) cytogenetic location: Xp21.2–p21.1.
- F5
Dystrophin is a long, rod-shaped protein lining the inside of muscle cells
UniProt P11532: 3,685 aa; N-terminal actin-binding domain, central rod domain of 24 spectrin-like repeats, cysteine-rich + C-terminal domains.
- F6
Dystrophin links the internal cytoskeleton to the extracellular matrix via the dystrophin-associated protein complex (DAPC)
DAPC: dystrophin binds F-actin intracellularly and β-dystroglycan/sarcoglycan complex at the sarcolemma, which binds laminin-2 in the ECM. Mechanical link preventing contraction-induced membrane damage.
- F7
1986: Louis Kunkel's group isolated the DMD gene by positional cloning
Monaco AP et al. Nature 1986;323:646-650 and Kunkel LM et al. Nature 1986;322:73-77: cDNA isolation from X chromosome walking; disclosed the gene's extraordinary size.
- F8
1987: Eric Hoffman identified the protein and named it dystrophin
Hoffman EP, Brown RH Jr, Kunkel LM. "Dystrophin: the protein product of the Duchenne muscular dystrophy locus." Cell. 1987;51(6):919-928.
- F9⚠ commonly confused
Two boys with similar-sized deletions can have very different severity: Duchenne (severe) vs Becker (mild)
The phenotypic split is real and well-documented; the reading frame is the key variable, not deletion size alone. Severity correlates with whether the deletion is in-frame or out-of-frame. Trap: do not imply deletion size alone determines severity — it does not.
- F10
The reading frame rule: severity determined by whether the remaining exons are in-frame or out-of-frame
Monaco AP et al. Genomics. 1988;2(1):90-95: "An explanation for the phenotypic differences between patients bearing partial deletions of the DMD locus." — this small paper proposed the rule in a proof-of-concept cohort. Large-scale validation (~91% accuracy) came later from Koenig 1989 and the Leiden DMD database (see F12). The narration does not cite a percentage.
- F11
DMD gene has 79 exons
PMC5664101 (L12, confirmed via paperclip): "The gene is comprised of 79 exons."
- F12⚠ commonly confused
In-frame deletion → truncated but functional protein (Becker); out-of-frame deletion → no protein (Duchenne)
The reading frame rule holds in ~90% of deletion cases (not 100% — some exceptions exist due to cryptic splicing and tissue-specific isoforms). Narration says "the protein lost entirely" for out-of-frame, which is the predominant mechanism in muscle; Dp71 and other short isoforms from downstream promoters can persist in non-muscle tissue but are not sufficient to prevent muscle disease. ⚠️ Attribution note: Monaco 1988 proposed the rule conceptually; the ~91% accuracy figure comes from large-cohort validation (Leiden DMD Database — Tuffery-Giraud et al. 2006, PMID 16770791). Narration does not cite a percentage so this is fine.
- F13
Without dystrophin, contraction micro-tears the sarcolemma
Contraction-induced membrane damage is the primary pathomechanism in DMD; demonstrated by Evans Blue dye permeability and serum CK elevation.
- F14
Muscle is replaced by fat and connective tissue (fibrosis)
Progressive fibrofatty replacement on MRI and histology is the hallmark of DMD natural history.
- F15
Boys with Duchenne typically lose independent walking in early teens
Average age of loss of ambulation: ~9-12 years without corticosteroids; with deflazacort/prednisone, typically extends to early teens.
- F15b
Duchenne is the most common fatal childhood muscular dystrophy
PMC5664101 (L12, confirmed via paperclip): "the most common inherited muscle disease in childhood." Emery 1991 classifies it as the most common fatal inherited muscle disease in childhood.
- F16
Before steroids, median survival was mid-twenties
Pre-corticosteroid era: median survival ~19–25 years (respiratory failure predominating). With modern care: median survival extending into 30s–40s.
- F17
Exon-skipping concept: skip an exon to restore reading frame (DMD → Becker-like)
Antisense oligonucleotide-mediated exon skipping to restore reading frame; concept validated in DMD patient cells and mouse models.
- F18⚠ commonly confused
Eteplirsen (EXONDYS 51), targeting exon 51, was FDA-approved 2016
fda_30f998aef14d (L8, L21, L28, confirmed via paperclip): "Approval Date: September 19, 2016" and "NDA 206488 / ACCELERATED APPROVAL." Trap: this was a controversial accelerated approval — FDA overrode its advisory committee. Approval based on dystrophin increase as surrogate endpoint; clinical benefit unconfirmed at approval. Narration says "approved in 2016" — factually correct. Three additional ASOs confirmed by PMC11818380 (L19): golodirsen and viltolarsen (exon 53) and casimersen (exon 45). Script's "Three more" = 4 total = correct.
- F19⚠ commonly confused
Delandistrogene moxeparvovec (Elevidys) approved by FDA 2023 as gene therapy
fda_3cd513537fb5 (L55, confirmed via paperclip): CBER Director memo concludes "accelerated approval … for the treatment of individuals ages 4 through 5 years with DMD." BLA 125781, June 22, 2023. Mechanism: AAVrh74 vector delivering micro-dystrophin (~1/3 size of full dystrophin). Full traditional approval for ambulatory ≥4 yrs: June 20, 2024 (separate expansion). Trap: initial 2023 approval was for ages 4–5 only, ambulatory; 2024 expanded to ≥4 yrs. Narration says "2023" — accurate for the first approval.
- F20
Guillaume Duchenne de Boulogne first described the disease clinically in 1868
Duchenne GBA. "Recherches sur la paralysie musculaire pseudohypertrophique ou paralysie myo-sclérosique." Arch Gén Méd. 1868 — the definitive clinical description. (First cases noted ~1858; full publication 1868.)